|
The AIDS Cure

Reservoirs of HIV hide deep within the body. Scientists are now closing in on methods to wipe them out. In 2007, a little-known German doctor applied to speak at a prestigious AIDS conference, claiming to have cured a single case of the disease. He described a 41-year-old man, dubbed the “Berlin patient,” who had had both AIDS and leukemia. The patient received a bone-marrow transplant from an HIV-resistant donor and no longer showed any sign of the virus. Perhaps the conference organizers didn’t know what to make of the case. They asked the doctor, Gero Huetter, to present the results on a poster instead of in a talk. So he did. The poster ended up hidden toward the back of a room. “I ran into the poster by mistake. No one was paying attention to it; there was no buzz,” says Stephen Deeks, professor of medicine at the University of California at San Francisco. Deeks was blown away by the poster’s claim and recalls thinking, “Why does no one seem to care about this remarkable case?” He moved on and didn’t discuss it with any of his colleagues. Weeks later, Jeffrey Laurence, a researcher at Weill Cornell Medical College, stumbled across Huetter’s abstract in the conference program. As the first author of a seminal 1984 paper showing that HIV causes AIDS—a controversial idea at the time—Laurence was all too familiar with the deadening silence that can greet revolutionary discoveries. He wanted to believe Huetter’s claim, and so in his role as a consultant for AmfAR, The Foundation for AIDS Research, he organized a think tank of 12 people in September 2008. Huetter was there, as were Deeks, Harvard University immunologist Judy Lieberman, and David Margolis, a leading AIDS researcher at the University of North Carolina. After scrutinizing the evidence, this jury of sorts unanimously decided that the Berlin patient, by then identified as Seattle native Timothy Ray Brown, was indeed cured of AIDS. “It was absolutely a turning point,” says Deeks. Until then, the best scientists had hoped for was to control HIV infection by impeding the virus’s ability to reproduce. Brown’s case galvanized them into action. There are now dozens of labs investigating how to eliminate HIV from the body entirely. Several companies are developing techniques that mimic the genetic mutation that made Brown’s donor resistant to the virus; a handful are now in clinical trials. Funding agencies have changed course as well. In December, the National Institutes of Health (NIH) announced it would dedicate $100 million over the next three years to accelerate such efforts. “It’s a huge shift,” says Nobel Laureate David Baltimore, who is spearheading one of the new trials. “There is a real recognition that it’s possible that we can get a cure.” Even among intractable diseases, AIDS is particularly challenging. It starts with HIV (human immunodeficiency virus), which embeds itself in a victim’s DNA. Once infected, cells cannot get rid of it, as they can most other viruses. What’s more, HIV targets cells in the immune system, converting them from disease fighters into mini factories, which then churn out more copies of the virus. Months or years later, the number of immune cells drops so low that a person becomes susceptible to all sorts of opportunistic infections and develops AIDS (acquired immune deficiency syndrome). If taken early enough, antiretroviral medication can prevent AIDS by keeping HIV levels in check, and there are more than 30 drugs designed to do that. Brown began taking antiretro-virals when he was diagnosed with HIV in 1995. Ten years later, he developed an unrelated case of acute myelogenous leukemia and deteriorated so rapidly that he soon needed a bone-marrow transplant. Bone marrow is the source of all of the body’s blood and immune cells, so a transplant essentially replaces the old immune system with a new one. Huetter, Brown’s hematologist, recalled reading about a genetic mutation that prevents HIV from infiltrating cells. Called CCR5-delta32, it’s a mutant form of CCR5, a receptor that HIV needs to gain entry into one of its well-known targets: CD4+ T cells. The mutation occurs naturally in only about 1 percent of people, and Brown was lucky enough to find a matching bone-marrow donor who carried it. “I was told that if I got his stem cells, it would probably take care of my HIV,” Brown says. “I thought, ‘That would be nice,’ but I didn’t really believe it.” Before his bone-marrow transplant on February 6, 2007, Brown underwent a punishing regimen of chemotherapy and total-body irradiation to wipe out his immune system. Two weeks later, he left the hospital with someone else’s. “That was the beginning of my new life,” he says. Huetter’s original treatment plan called for Brown to continue taking antiretroviral drugs after the procedure. But Brown says his partner at the time, a massage therapist, had an “intuition” that the stem cells from the transplant wouldn’t reproduce properly if flooded with the chemicals. The transplant team was likewise reluctant to risk damaging the fragile new cells, says Huetter, and so Brown went drug-free. After the first few months, it slowly became clear that even without the medication, Brown showed no sign of HIV. Other cases have since emerged that hold similarly tantalizing promise. Last March, a team of scientists reported that a three-year-old girl born with HIV in Mississippi remains free of the virus months after she stopped aggressive therapy. And French researchers published results showing that 14 people (now 19) who had been treated with antiretrovirals within 10 weeks of being infected have remained healthy for years after going off the drugs—more than 11 years in one instance. Of these cases, only Brown has had a follow-up long and thorough enough—including brain, gut, colon, and lymph-node biopsies evaluated by multiple labs—to merit the unequivocal label of “cure.” But bone-marrow transplants are hardly an option for the 34 million people infected with HIV worldwide: They’re arduous and highly risky procedures-; up to one third of transplant recipients don’t survive. The transplants may not even work consistently. In July 2012, doctors announced that two men in Boston seemed HIV-free following bone-marrow transplants like Brown’s. But unlike Brown, the men had remained on antiretroviral therapy after their procedures. When they stopped taking the drugs early last year, their infections came roaring back. It’s not yet clear why—whether it’s because their transplants didn’t come from HIV-resistant donors, or because their pretransplant treatment didn’t eliminate all of the infected immune cells, leaving some HIV hiding out in the body. Still, Brown’s case offers hope. It is evidence of something that until recently had been only a theory: that even after many years of infection, when HIV has presumably wormed its way deep into a person’s body, it is possible to eliminate it entirely, given the right approach. HIV tests typically measure the amount of viral RNA in the blood. If you imagine blood vessels as highways, with some number of cars, or HIV-infected CD4+ T cells, traveling along them, the tests essentially try to extrapolate the number of cars on the road into the number of cars in the whole country. The problem with this logic, says Mike McCune, professor of medicine at the University of California at San Francisco, is that there may be only a few cars on the highways because people have chosen not to drive, or gas stations have run out of fuel, or the factories that make the cars have been bombed. In fact, in 1995, a team led by Robert Siliciano at Johns Hopkins University School of Medicine found that the vast majority of HIV hides silently in “resting” CD4+ T cells. When people go off therapy, the virus from this latent reservoir of infected cells rapidly resurges. In the analogy, this means that cars are idling in garages, waiting for an opportune moment to pull out. But even that is probably not the whole picture. For example, scientists have begun to realize that the reservoir contains other types of infected immune cells, such as dendritic cells, monocytes, and macrophages. In October, Siliciano and his colleagues reported in the journal Cell that the reservoir of resting CD4+ T cells alone may be up to 60 times larger than was previously thought. Perhaps the biggest obstacle to curing AIDS, then, is this: No one knows what the reservoir is, where it is, or how to rouse the latent virus from it, much less how best to determine that it has been eradicated once it has been roused. These questions have prompted a tremendous amount of research, with scientists around the globe studying as many infected tissues as possible, both in people and animal models. So far, one of the most popular strategies for obliterating the reservoir is the “shock and kill” approach. The goal is to somehow jump-start the dormant virus into becoming active, and then destroy the infected cells once they’re vulnerable—in other words, lure the cars out of the garages and onto the highways, and then blow them up. Of the three AIDS research collaborations the NIH has recently funded, one focuses on this approach; academic researchers and the pharmaceutical giant Merck hold weekly calls to share unpublished results. “The idea is to find agents or small molecules or drugs that can reverse latency,” says Janet Siliciano, a virologist at Johns Hopkins University and a member of the group. “That’s a really, really hard problem. Right now there’s nothing out there that’s doing that.” Brown’s case, she says, “created huge, huge excitement. It was a proof of principle that you could eliminate the reservoir if you could give someone a bone-marrow transplant.” The Mississippi baby was given antiretroviral drugs starting at birth, and the most popular theory is that she was treated so early that the HIV reservoir never had a chance to fully form. The group of patients in France had also been treated soon after infection. As a result, their reservoirs may be so small that their immune systems can control the virus. The French researchers estimate that as many as 15 percent of patients who receive similarly early intervention may become “elite controllers”—a concept akin to that of cancer remission. But Robert Siliciano cautions that these are unusual cases. “In most people, we’re going to have to deal with this reservoir somehow or other,” he says. “We’re not going to cure anybody unless we get rid of it.” Scientists have known for many years that HIV’s dependence on the CCR5 receptor might prove to be its downfall. Brown’s case has given that hypothesis new momentum. Two California companies, Sangamo Biosciences Inc. and Calimmune, are using gene-therapy techniques to disable or delete CCR5. In Calimmune’s trial, researchers take blood from an HIV- infected person, isolate stem cells, disable CCR5, and then transplant the stem cells back into that individual, where they will develop into new immune cells. Theoretically, this approach has two advantages: The stem cells provide a steady stream of HIV-resistant immune cells, and altering a patient’s own stem cells rather than those from a donor circumvents the risk of rejection. The trial kicked off last summer, however, so it’s too soon to say if the strategy is as powerful in practice as it is in theory. Sangamo’s approach is further along. It also modifies CCR5 but in T cells, which is easier to do. The company uses molecular scissors called zinc-finger nucleases to snip both copies of the CCR5 gene out of an HIV-infected individual’s T cells. Researchers then grow the modified T cells to large numbers and transplant them back into the patient. In a trial of nine people, Sangamo found that a single infusion of the engineered T cells shrank the size of the reservoir in all of the participants three years later. In a separate trial of eight people, one person has maintained undetectable levels of the virus for 20 weeks (as of December) after stopping therapy. “This is the first study to show a long-term durable increase in CD4 counts but a concomitant reduction in the reservoir,” says Geoff Nichol, Sangamo’s executive vice president of research and development. Still, it’s way too early to say whether this effect will persist. Because T cells have a limited life span, it’s not clear how long a single infusion’s benefits will last. Sangamo is planning to apply the same technology to stem cells, which might be able to provide an unending supply of HIV-resistant T cells. A more interesting question is why this approach should have any effect on the latent reservoir—that is, why should an infusion of healthy immune cells decrease the number of cells that are already infected? One controversial idea holds that the reservoir isn’t entirely dormant. Imagine the reservoir as a sink half-filled with water. Each day, the water level is exactly the same as on the previous day. “But what you didn’t realize is that the faucet’s a little bit open, and the drain is also a little bit open,” says Mario Stevenson, professor of medicine and chief of infectious diseases at the University of Miami. So even though the water level seems unchanged, there is fresh water in the sink. In the same way, the reservoir may be dynamic, with some cells getting infected and others dying every day. In a person infused with the engineered T cells, the virus would gradually kill all infected cells without infiltrating new ones. In a sense, “you allow the infection to proceed untreated until the virus itself eliminates all of the nonengineered host cells,” says Deeks. “It’s a pure Darwinian experiment.” Even if Sangamo and Calimmune’s approaches prove successful, and even if they turn out to have no serious side effects—and these are big ifs—they are too expensive and invasive to treat everyone infected with HIV. In fact, experts all seem to agree that any global strategy for eradicating HIV may need to combine a cure with a vaccine. After decades of failure with candidate vaccines, that field, too, has seen promising developments. For example, after working with only a handful of neutralizing antibodies—immune molecules that can drive a vaccine—Dennis Burton and his colleagues at The Scripps Research Institute introduced two powerful new ones in 2009. That catalyzed an explosion of others. “Now there are literally hundreds,” says Burton, a professor of immunology and microbial science. Researchers have also created vaccines that spur healthy T cells to attack HIV-infected cells. They’ve shown dramatic protection in a monkey model of AIDS. And last October, scientists revealed the elusive structure of the protein protruding from HIV that the virus uses to latch onto CCR5. This protein is a target for antibodies elicited by vaccines. Put all of this together, Burton says, and “you start to glimpse the possibility of controlling or even eradicating the virus.” In the meantime, Brown still holds the distinction of the first and only confirmed patient cured of AIDS. He has some survivor’s guilt, he says, and is often called “lucky” by HIV-positive individuals. But his recovery was speckled with a series of nightmarish scenarios: At various points, he was incontinent and unable to walk, placed in an induced coma because of an acute sepsis infection, and so delirious he had to be admitted to a hospital for people with severe brain injuries. Through all this, Huetter’s team kept testing Brown and couldn’t find any trace of HIV. But Brown says he didn’t really believe his extraordinary situation until the New England Journal of Medicine published his case report in 2009. “Then I thought, ‘Okay, the medical establishment is accepting that I’m cured,’ ” he recalls. “I guess I’m cured.” The Youth CorpsEach year, an estimated 250,000 children worldwide are born infected with HIV. What if hundreds, maybe even thousands, of them are now free of the virus and don’t know it? This is the hope that the case of a baby in Mississippi offers. The baby was born to an HIV-positive mother and received antiretroviral drugs within 30 hours. Normally, when a baby is diagnosed as HIV-positive, he or she begins treatment and continues it indefinitely. But the Mississippi baby stopped getting the drugs when she was about 15 months old. By the time she returned to the health care system, she had been off therapy for about a year. Instead of being desperately sick, she showed only a faint trace of HIV. This discovery has led to speculation that the antiretroviral drugs killed off all of the virus before it had a chance to form a reservoir. To test whether that’s plausible, some groups are embarking on ambitious projects to treat infected newborns within a day or two of birth, discontinue treatment after one or two years, and then monitor them to see if the virus rebounds. “Essentially the plan, based on the Mississippi baby, is going to be: Can you replicate this under controlled conditions in a larger number of people?” says Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases, which is funding one such trial. If doctors follow enough of these children over time, they may eventually be able to verify that they are cured, Fauci says. Other groups are looking to see whether HIV-positive teenagers who go on “drug holidays” and temporarily stop taking medication remain free of the virus. “The first step is remission. Maybe cure will be the next one,” says Christine Rouzioux, a virologist at Necker Hospital and University of Paris Descartes in France. “It’s the beginning of the story.” Update: On Wednesday, scientists announced that a second baby may have been cured of HIV. How HIV Invades Cells—And How To Stop It 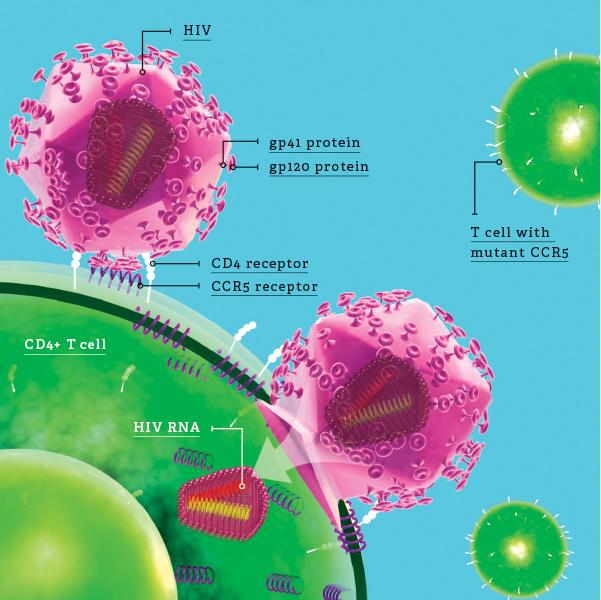
HIV Invasion
Don Foley 1) HIV attacks immune cells that express a surface receptor called CD4. The best known is the CD4+ T cell. First, the gp120 portion of a protein protruding from the viral envelope, or virus’s outer coat, latches onto CD4. 2) The binding triggers a structural change that exposes another viral protein, gp41. This protein docks with a second surface molecule called CCR5 (or for some cell types, another co-receptor called CXCR4), which enables HIV to penetrate the cell’s membrane. 3) The virus then releases its genetic material, which embeds itself in the cell’s DNA. The infected cell either begins churning out copies of HIV or silently waits to be activated. 4) Immune cells that carry a mutant form of CCR5 don’t allow HIV to bind. Several research groups are trying to mimic this natural resistance by introducing mutant versions of CCR5 into HIV-infected people. This article originally appeared in the April 2014 issue of Popular Science. Source: PopSci
Share this with your buddies. You know they want to get smashed.
|
We Share Stories Like this Every Day
Follow us to get your Daily Tech Recap! Latest Geeky Goodness:

This Bird feeder is definitely Squirrel Proof

The Diving Bell and the Exoskeleton: An Excursion into the Depths

Canary raises $10 million for app-enabled home security

How to Make a No. 1 App With $99 and Three Hours of Work

E-cigarette ban for Los Angeles
Flipboard Acquires Social Magazine Zite From CNN

Is this a bike, a skateboard or just downright stupid?
Reenact 'Jurassic Park' hacking scene

This Robot plays Flappy Bird, and it's pretty good too!

A look back at technology we wish had worked: The Rocket Belt

Is the Internet watching you sleep? The perils of unsecured webcams: The last one is just SHOCKING.

How the web was born: WWW turns 25

Scientists get a shark's eye view using wearable computers

What the hell is this giant Russian car?
The Tech Industry Is Completely Ridiculous. Let’s Hope It Stays That Way

Insane tower design launches people on an awesome roller coaster loop
|
| Recaply Copy |
|
